Anatomy of a Sarin Bomb Explosion (Part II)
Translations:
Introduction
Part I describes the basic behaviour and intended function of an air-delivered gravity bomb containing Sarin, designed along US/USSR cold war lines. When we left off in Part I, a well-crafted gravity bomb will have dispensed its Sarin broadly along this distribution:
- Aerosol: The majority of the contents will have been dispensed as a finely divided mist of small droplets.
- Vapour: A small amount of Sarin will be in vapour state from the elevated temperature of the explosion.
- Liquid: Some Sarin will be in liquid form in the crater and immediate vicinity of the explosion, having been dispersed in drops too big to form an aerosol. Other bits of liquid are likely to be on the surface of fragments of the bomb.
- Destroyed/Decomposed: A non-trivial percentage of the Sarin will have been destroyed by the explosion, or even have degraded before the bomb was used.
How does Sarin Work?
Sarin, also commonly known by its old NATO nickname GB, is one of a family of chemical warfare agents known as nerve agents. It was invented by German scientists in 1938-1939 who were performing research on organophosphorous pesticides led by Dr. Gerhard Schrader. Sarin was named by the team of researchers who invented it. It is in a family of chemicals known as organophosphates. There are other chemicals within this family, including the chemical warfare agents Tabun, Soman, VX, and the pesticides Malathion, Parathion, and Amiton.
All of the nerve agents affect the human body’s nervous system. The human nervous system requires a delicate balance of chemicals to regulate itself. Nerve agents bind to a chemical known as acetylcholinesterase and, in doing so, disrupt the electrochemical reactions required for the body to operate properly. The binding of acetylcholinesterase leads to a build-up of acetylcholine, which then in turn leads to a syndrome called a “cholinergic crisis”. In effect, the nervous system starts to over-act and muscles and glands start to work over-time and cause serious problems. The signs and symptoms will vary in severity and timeline depending on the route of exposure and dose (i.e. the amount of Sarin absorbed). This will be discussed at length below.
Routes of Exposure: How can Sarin enter the human body?
There are several ways Sarin can enter the human body. These are called “routes of exposure” and are as follows:
- Respiratory: Sarin in vapour or aerosol form can be inhaled.
- Ocular: Sarin can be absorbed by the eyes.
- Dermal: Sarin in liquid form, or a very high concentration of aerosol or vapour (many times higher than that which is lethal through inhalation).
- Via Wound: Through a disruption in the skin. This would generally only occur if Sarin in liquid form was on a fragment or sharp object and it entered into the human body. This is a rare scenario.
- Gastrointestinal: Sarin can enter the body if ingested. This would happen if it was in food or drink, for example. However, Sarin rapidly degrades in the presence of water and moisture, so this is also a fairly exotic scenario.
Sarin acts very quickly through respiratory and ocular exposure, with onset of adverse effects within seconds to a few minutes depending on dose. Absorption through the skin is slower, i.e. minutes to hours, depending on dose. Rate of action for wound exposure is believed to be intermediate in speed between respiratory and dermal absorption. Gastrointestinal absorption is not well documented but is likely to be fast.
Sarin, as it is less persistent and evaporates at a faster rate relative to the other nerve agents, is foremost an inhalation hazard. Absorption through skin takes time, and even someone with liquid Sarin on their skin is extremely likely to suffer inhalation effects from the Sarin evaporating off of their clothing and skin, except in very cold weather. In moderate or warm temperature situations, the only realistic exposure scenarios for a “liquid Sarin only, through skin absorption” are for partially protected troops already wearing protective masks or donning them very quickly at the onset of a chemical attack. So, with unprotected target populations, the route of exposure of most significance is inhalation of aerosol and vapour.
Signs and Symptoms:
The “cholinergic crisis” that Sarin (and its other cousins in the same family) provokes manifests itself in signs (things that are externally observable) and symptoms (subjective indications felt by the victim that are difficult or impossible to observe). This graphic, taken from the canonical Medical Aspects of Chemical Warfare (various editions accessible online) lists the major signs and symptoms:
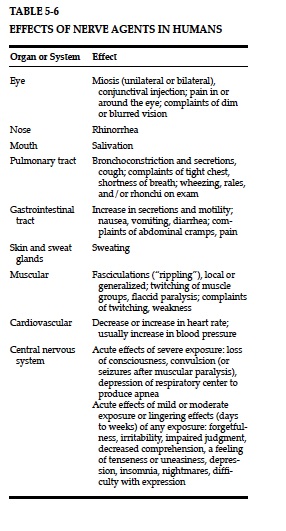
Rhinorrhea is a fancy term for a profusely snotty nose. Miosis means pinpointing of the pupils. The rest is either self explanatory or you can look it up in a normal dictionary if unsure.
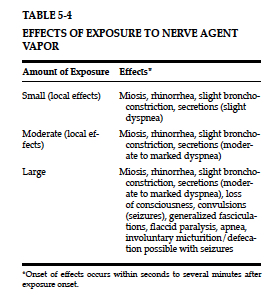
The order in which signs and symptoms appear and their severity will vary both with degree of exposure and route of exposure. For Sarin, this is principally inhalation. This graphic describes this exposure category in detail:
In the event of liquid absorption through skin, signs and symptoms progress differently. This is really more relevant for the more persistent, slower evaporating agents like Tabun and VX. In the case of Sarin exposure, an unprotected person with lots of Sarin liquid on them will get respiratory exposure from evaporation, and this is very likely to happen faster than dermal exposure. With Sarin, the likely exposure scenario is for someone who has protective equipment for their respiratory tract and eyes (e.g. a gas mask) but unprotected skin. For comparison purposes, this is the progression of signs/symptoms for dermal exposure:
When people die from nerve agent exposure, the mechanism of death is almost always a pulmonary death. Such respiratory failure, which denies the body oxygen happens through several mechanisms with nerve agent poisoning. Depending on route of exposure and dose, any or all of these will be the exact mechanism by which death occurs:
- Bronchoconstriction – narrowing of the air passageways in the lungs
-
Bronchorrhoea – buildup of water sputum in the respiratory tract
-
Central Apnea – the brain stops sending signals to breathe.
- Paralysis of the muscles needed for respiration
All of these conditions can cause cyanosis , a tell-tale blueish discolouring of skin due to oxygen deprivation.
What levels of Sarin are dangerous?
Most studies of the toxicity of Sarin are derived from data involving animal research. Much of the information is now quite dated, having been developed in the 1950s and 1960s. These should all be taken with a reasonable margin for error. However, the following chart from the US Army’s Field Manual 3-11-9 is as useful a summary as any I’ve seen. Anyone interest in the footnotes can go to the Field manual and look them up, although some of the references are to studies and documents not readily available online. You might need a good research library.
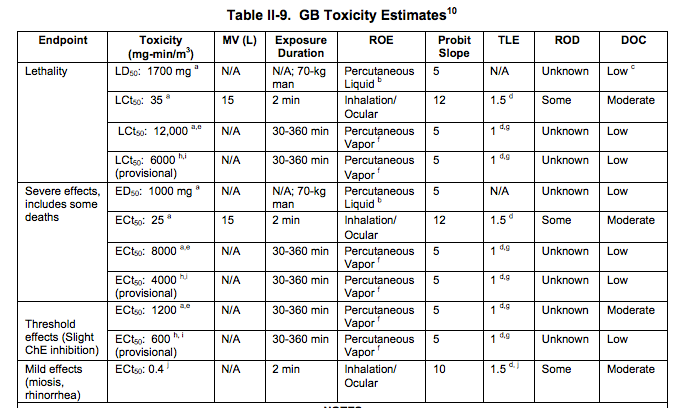
Unpacking the numbers
These numbers probably mean little to most readers so I am going to unpack this at some length. Concentration is measured in milligrams per cubic meter. As there is almost nothing in toxicology that’s instant, concentration is measured over a time domain. So for things like vapor exposure, the figures used are in milligrams per cubic meter per minute. For example 50 mg-min/m3 means 50 mgs of Sarin per 1 cubic meter of air for a period of 1 minute.
Toxicity by inhalation
The key figure here is something called 50th percentile Lethal Concentration – LCt50. This is the concentration that is reckoned to kill half of the exposed population, assuming a normal adult male (these studies were all based around Cold War soldiers) breathing at 15 liters of air per minute. This is the MV (‘respiratory minute volume’) on the table. This is equivalent to a soldier engaged in moderate activity. (Someone asleep will be breathing slower, someone running full tilt is likely to be higher.) So, for Sarin, breathing 35 mg Sarin in aerosol or vapour, per cubic meter of air, continuously for 2 minutes, will kill about 50% of the exposed people. This is extremely lethal. By comparison, the similar figure for phosgene, the most lethal chemical weapon used in World War 1, is about 1500 mg-min/m3.
For severely debilitating effects, the figure for Sarin is 25 mg-min/m3, again over the course of 2 minutes, not much less than the lethal figure. It is likely that there would be some lethality at this level. For mild effects, the threshold is around 0.4 mg.
Toxicity by absorption of vapour/aerosol through skin:
Sarin vapor and aerosol can enter through the skin. However, if you examine the table, these effects require a FAR HIGHER level of concentration and longer exposure. Lethal concentrations (LCt50) for this route of exposure are 6000 to 12000 mg-min/m3 for much longer durations of exposure (30 mins to 6 hours). This is an entirely difference exposure scenario. (The differences in the figures in the table are for differing air temperatures.) So, yes, Sarin is lethal through a route of permeation through the skin, but only at levels that are literally hundreds of times higher than the levels that are dangerous for respiration. The figures for severe effects (4000-800) and minor effects (600-1200) are correspondingly lower, but still MUCH HIGHER than effective concentration levels for absorption via the respiratory route. It should be noted that a very dense aerosol may result in some condensation or deposit of liquid on skin, which behaves as described in the next paragraph.
Toxicity by absorption of liquid on skin:
Percutaneous liquid exposure takes time, as was noted above. Time of exposure is a bit different here, and is less significant than the amount absorbed through the skin. A large gob of Sarin landing mostly on outer clothing and almost instantly removed by decontamination may result in less net absorption of Sarin into the body than a small droplet on the back of the neck that goes unnoticed until symptoms appear.
LD50 for Sarin is calculated at 1700 mg for a 70 kg male. This means that, for a normal 70kg human male, 1700 mg of Sarin absorbed into the human body would kill about half of the people with that level of poisoning. Statistically, some would die with less, and some could survive with a much higher exposure. ED50 is the level of exposure for serious, disabling effects. For Sarin it is 1000 mg for the same assumptions. Note that at this level of dose, some are likely to die. This is an awful lot of Sarin when compared to the amounts that are needed to kill or seriously incapacitate people through inhalation.
The behaviour of Sarin on skin is important. Several things happen when Sarin is on human skin:
- Some of it is absorbed through the skin into the human body. This Sarin does not readily come back out of the human body. It is busy binding itself to chemicals in the nervous system. Rather a lot of it is degrading in the blood stream into other things, as the blood is still largely water. But there is not a ready mechanism for Sarin that has been absorbed in the body to come back out and be harmful for others.
- A lot of it evaporates, depending on temperature, both of the skin and ambient temperature of the environment. Due to proximately of the mouth and nose, this means that Sarin on skin may be more acutely a respiratory hazard than an absorption hazard.
- One of the more immediate effects is the stimulation of sweat glands. Even low level exposure to Sarin can produce much sweating. However, sweat is largely water. And Sarin is both water soluble and reacts with water to break down into less hazardous substances. So, some Sarin on skin is likely to be removed or neutralised. This has not been well-studied and I do not know if this is a major or minor factor.
For those who are curious, here’s what some of the other columns mean:
- ROD – Rate of detoxification. The rate at which the human body can render the toxic substance safe.
- DOC – Degree of confidence. Basically, how accurate do the authors of the field manual believe these figures are.
- TLE and Probit Slope: These are mathematical concepts that are a bit complex for discussion here and have to do with how you extrapolate the given toxicity figures for other combinations of concentration and time. If you really want to get your head around this, see pages II-7 to II-9 in the Field Manual.
Applying this knowledge to field scenarios:
Now that we understand the practical toxicology here, it is easy to analyze exposure scenarios in the field. It is clear from the toxicological data that Sarin is far more efficient as a killer in an aerosol or vapour form, easily by several orders of magnitude. A weapon system that dispenses its contents in the form of liquid would largely be a waste of expensive Sarin. So, we are now understandably back to the concept of a weapon system that is designed and tested to optimize the quantity of aerosol.
In our suspected scenario in April 2017, there is a well-substantiated allegation that an air-dropped Sarin bomb was dropped. It appears to have functioned as designed and created an aerosol that drifted downwind, as the victims were a distance away from the bomb. Any person close enough to have been splashed with some liquid was probably close enough to the bomb to die very quickly. In any case, the impact point appears to be in the middle of a road.
So, for a person to be seriously ill or to die, there is a need to create an aerosol of a concentration of 25 to 50 mg-min/m3. So, people exposed to an aerosol of this density will get sick and easily could die. People exposed to an aerosol of only 2 or 5 mg-min/m3 may easily get very ill, particularly if they are in it for minutes. But think it through. A cubic meter is a lot of air. And that’s a very small amount of Sarin. How much Sarin is actually going to get deposited on their skin, hair, and clothing. A few milligrams, maximum.
Next, these people either escape or are carried away a significant distance and then receive emergency treatment. There are firm reports of responders going to rescue people becoming victims. However there are videos taken in locations some distance away from the impact site. People wearing little or no protective gear are seen handling the victims. Why are they not being seriously affected by Sarin? The simple answer is that these victims were affected by aerosol and/or vapour. Very little material actually got deposited on them. Even if it did, it would have been in the order of a few milligrams. And it takes 1700 milligrams over a period of time to kill someone by simple absorption. Responders aren’t falling over because, simply, the math doesn’t work and Sarin isn’t a magical substance.
Why then do emergency responders in more developed/better equipped situations train to wear full protective equipment? For several reasons. Emergency responders wear equipment that is prescribed through obeisance to occupational health and safety regulations, not a “what can I get away with and not die” ethos. Second, in the early stages of an incident, the chemical agent that was used may not be known. Even if you knew it was a nerve agent, you aren’t likely to know it was Sarin and not one of its more persistent cousins. VX, for example, is a different game altogether being primarily a contact/liquid hazard and requiring more skin protection when dealing with victims.
The bottom line is that Sarin evaporates quickly, not much is needed to do harm to people, and people who are exposed only to aerosol and vapour are a minimal contact or respiratory hazard to others. Even given this, some responders reported illness. So, the “Responders didn’t die on film so it wasn’t Sarin” is an incorrect line to take here and displays a basic ignorance of the facts.
